
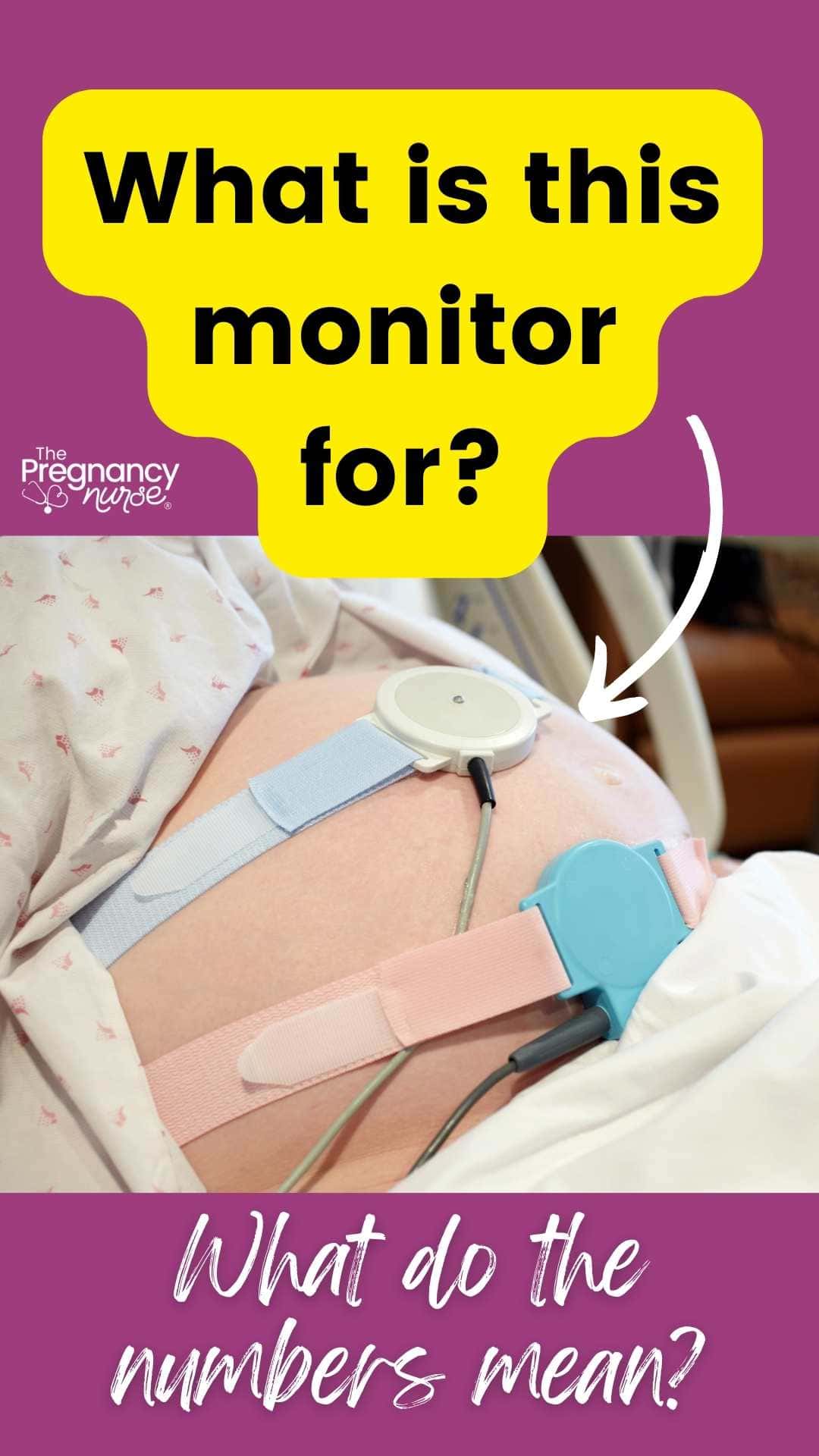
The toco is the monitor that measures contractions on the fetal monitor. It can be interesting to know how the reading correlates with how strong your labour is. But the big question is if those uterine contractions are pushing the baby into the birth canal — so, how does that correlate with the numbers on the monitor?

But, how the heck do I know so much about uterine contraction monitoring?
Hi, I’m Hilary — many people know me as The Pregnancy Nurse . I have been a nurse since 1997 and I have 20 years of OB nursing experience. I have spent lots of time in fetal monitoring classes, and have spent countless hours watching, counting, explaining and charting on fetal monitoring, so I’m a great resource on this. I am AWHONN fetal monitoring certified as well.
How do they Measure Uterine Contractions?
There are two different types of monitors that we use to monitor contractions in the fetal heart rate monitoring system.
Toco is normally a round monitor that we place on your belly and it is similar to a scale. Meaning, as your belly pushes up against the monitor it registers it — just like pushing weight down on a scale makes it register.
But, as you can imagine that it is on top of your uterus the number it registers includes a few things:
- What the monitor is at when the uterus is not contracting. Similar to how you “zero” (or tare) out a scale the nurses will need to zero the monitor when your uterus is not contracting to make sure it’s starting low. As you shift and baby shifts she may need to zero it again…
- Placement of the monitor can really adjust for how high it reads during a contraction. If it’s on a baby’s appendage (head, bum or elbow) it will register higher than if it’s on a softer spot of the uterus.
- The amount of muscle muscle/ skin / fat in that area. This can really make that number vary. But, sometimes super skinny ladies it doesn’t register as well…
I always tell my patients that fetal monitoring is an art not a science. It takes a lot of feeling, experience and sometimes luck to get the monitors in the right place for you & your baby.
There is also an IUPC — Intra Uterine Pressure Catheter — it’s a tube that we insert into your uterus (your water has to be broken to have an IUPC) and it lays between the uterine wall and the baby’s head and specifically measures your contraction strength. Since this is directly measuring the strength of the contraction it is more accurate.
The IUPC can also be used to run an amnioinfusion where they run saline into your uterus to help cushion baby, or possibly wash-out some meconium.
And yes, I talk more about (and show some videos/images) of both of those kinds of monitors in here.
So, as you can tell the specific number doesn’t matter quite as much. In fact in general we don’t even chart the number when we use a toco, we chart, mild, moderate or strong — and will report the same to your MD.
Really quick, if you’re like — this is interesting, what else should I expect at the hospital? — Come join me in here. It really is the easy way to get prepared and understand what will go on at the hospital — and you will be SO glad that you did!
Which one is the contraction monitor?
Normally, on a belly where the baby isn’t breech the contraction monitor will be above (closer to the patient’s head) than the fetal heart rate monitor.
On the print-out, normally the contraction monitor is the bottom line (that tends to have “hills” or “mountains” on it).
What’s the other monitor for?
While this article is all about monitoring contractions, there is another important part of this and that is the fetal heart rate monitor. That is a post all on it’s own and it is also much more complicated (and probably important). So, if you want a post about that — tell me in the comments!
The fetal heart rate is the upper line, and it is normally much more jagged with ups and downs (and all of that is pretty normal).
Remember that doing kick counts at home is your best indicator for fetal well-being, so be SURE that you’re doing those:

What Toco Reading is a Contraction?
So, as a nurse (who spends hours and hours and hours learning fetal monitoring) — what they’re looking for is a bump up from baseline.
They look like little hills (or bells) on the read-out. Sometimes those hills are giant, and sometimes they’re small However, as a nurse with a toco I can’t trust that, and I use my hands to push on the woman’s abdomen to see how strong the contractions feel (called palpation). It takes a lot of experience, and touching a lot of pregnant bellies, to become an expert in that. I also talk to them about what they are feeling. If a patient is feeling like the contractions are more painful, or if they have shifted where they feel (like front to the back) the and I take that into account as well.
A contraction normally sort of “puckers” your uterus pushing it out from your body as it squeezes on the baby — and it is that motion that is recorded on the toco monitor. Pucker your lips together, and you’ll kind of get an idea of what it is like, if the monitor was at the front of your lips.
What is the Braxton Hicks Toco Reading
This is where it gets tricky. As a nurse, sometimes you’ll look over at the fetal monitoring machine and people have giant contractions, but they aren’t feeling too much (check out my post on having contractions on the monitor that you don’t feel). And sometimes contractions are very painful (per the patient) and they register as very small.
And honestly, after 20 years all of that is super normal to me. I just adjust the monitor and keep asking questions and assessing the patient.
Braxton Hicks contractions don’t progress the baby into the birth canal (thereby opening the cervix). So, the only real way we can know that they are not Braxton Hicks is by checking your cervix to see where baby is (and possibly checking it again to see what they are doing to your cervix).
They can read at any number on the monitor, and actually people can report them to be very painful when they rate the intensity — but it really depends on how they are pushing down on baby.
Some Braxton Hicks are very mild, and patients just report them as “tightening” but some say they are very painful and I tend to figure that the uterus just doesn’t have it’s act together in a motion to push the baby DOWN towards the birth canal yet. Don’t worry — it will figure it out.
Ok, I am loving that you made it this far into this article — it really shows you’re ready to LEARN about your birth. The thing is, you don’t know what you don’t know — which is why I recommend EVERYONE take a class that goes beginning to end. I once had a study that said you only use about 20% of what you learn in class, but everyone uses a different 20%, so you’re not sure what you need. I think that’s so true.
The good news is that The Online Prenatal Class for Couples really prepares you in a quick way, so you’re prepared and on your way (rather than being tortured by a class). I 100% recommend it, and I love that couples do it together so they are BOTH prepared. There’s nothing smarter than that!
What Toco Number is a Strong Contraction
Again, we don’t give it as an exact number when we are talking about the TOCO — mostly because that baseline number (like when you zero a scale) is often all over the place as you move and baby moves. As I’m sure you could imagine that if your baseline is at 50 and the contractions are going up to 70 it’s different than if the baseline is at 20 and the contractions are up to 70 (and she’s skinny and the monitor is in just the right place).
However, with the IUPC we get into a spot where we can tell (more) about how strong the contractions are, and similar to blood pressure it is measured in milimeters of mercury (mmhg). We measure how many contractions you have and how high they go (minus’ing the baseline number where it’s at when you aren’t having a contraction) and we get a number we call Montevideo units. We want those to be at about or above 200 in a 10-minute time period to show that you’re in good labor.
Montevideo units can be more important when you are having an induction of labor (because we need to know if the Pitocin is enough to make your uterus contract enough).
If you were to have contractions, and they seem to stall out and you’re not progressing, they often will insert an IUPC to make sure that the contractions are adequate to make your cervix open. If you were to be having those adequate contractions without any changes in your baby’s position or cervix we’d have to consider what’s going on at that point.
Contraction monitoring FAQ
Toco Monitor Reading 20 What’s That Mean?
It can mean that the “Baseline” is at 20, or if it rising to 20 from a lower number then it is likely a contraction, and through palpation and what you report we’d count is as mild, moderate or strong.
The question is really the SHAPE of the line.
Fun fact, sometimes even the contractions will extend below the baseline depending on where we place the monitor. We’re really just looking for the “hills” on that monitor, whether they go up or down. AND we also use the patient’s experience to understand what is going on.
You can sometimes even count a patient’s respirations on the monitor as well — it’s normal for that number to go up and down about 5 with the patient breathing.
What Type of Monitoring Is Best for You?
If the question is between the IUPC or the toco, if your water hasn’t broken yet most often a TOCO is what is best. However, if things aren’t progressing an IUPC can give you more information about what’s happening in the womb and how contractions are actually happening.
But, remember they have to break your water to insert an IUPC (but they do that if necessary).
If you have any questions about what is best for you, be sure to talk with your providers about what is going on and what the risks, benefits and alternatives are. The chapter on provider communication in here is super helpful in that case.
How effective is uterine monitoring?
Uterine monitoring is a procedure used to monitor the labor and delivery process during pregnancy. It involves monitoring uterine activity, cervical changes, and fetal well-being as labor progresses.
I want to be clear that as nurses and doctors/midwives — we don’t just take the #’s on the screen as uterine monitoring, it also involves patient reporting, and our feeling the patient’s abdomen.
Uterine monitoring can help detect any signs of preterm labor or other complications that may arise during childbirth.
When combined with monitoring baby’s heart rate, it can help identify any changes in fetal heart rate that could indicate distress or an unusually rapid rise in fetal heart rate that could be cause for concern.
The readings taken from uterine monitoring should always be interpreted by a trained medical professional who can accurately assess the patient’s condition and provide appropriate care if needed.
Studies really show that fetal monitoring in general is best for those in active labor, or those being induced. Which, is why we try to encourage people to stay home more if they aren’t in active labor yet (I have a whole post on when they’ll admit you for labor).
What is the Y Axis of Fetal Monitoring?
The Y access it the numbers going up on the graph.
They show baby’s heart rate, and also the TOCO pressure numbers or IUPC numbers.
The X Axis of Fetal Monitoring
The X axis measures time, smaller boxes are minutes, and usually a more bolded line is 5 or 10 minutes. We use these most with contractions to tell us the frequency, or how many minutes apart the contractions are.
Do they always print the fetal monitoring?
Not always, in fact during Covid there was a shortage on the paper so hospitals were trying to conserve it as much as possible.
Do you and your partner 💑 want to be more prepared for your upcoming delivery? This is for you!
Hospitals are required to save the fetal heart tracing strips somehow on the “cloud” for a number of years when done either via paper or electronically (and I believe they area also required to have even a secondary backup in case the previous cloud has an issue).
What Do Contractions Feel Like?
Contractions are the body’s way of preparing for labor. They are tightening of the uterus muscles and help to move your baby out and down into the birth canal. Contractions can be felt differently by different people, but they often start as a low and uncomfortable ache in your lower abdomen that gets stronger until it peaks and then slowly fades away.
The pain may radiate to your lower back or upper thighs, or you might feel pressure in the area between your vagina and anus. Your healthcare provider or midwife will be able to tell you what to expect when it comes to contractions during labor.
If you’re worried about the pain of contractions, and are wondering what your options are — come join me in The Online Prenatal Class for Couples. There are a few options and understanding them can help a lot!
Do you and your partner 💑 want to be more prepared for your upcoming delivery? This is for you!
A final word on reading contractions on a monitor
Remember, the number doesn’t really matter. It’s much more the pattern we see on the monitor, when combined with what you are experiencing (and what the contractions are doing to the fetal heart rate). This actually takes a while for new nurses to understand, but it is really important that we take into consideration:
- Proper positioning of the monitor (and I’ll admit sometimes it’s a crap-shoot for the nurse, and they have to move it a few times to get it right).
- Patient’s experience with the contractions
- How the contractions palpate for the RN.
- How baby’s progressing into the birth canal.
I hope you found that helpful. It really is all pretty easy to understand when you have someone who understands it and can easily explain it to you. That’s why I created The Online Prenatal Class for Couples where we prepare you for birth in just a few hours I’d love to have you join me!
Have you checked a birth class off your to do list✅? I have a few I recommend:
❤️ Best class for couples {per BabyList}
👩💻 Best class available on demand
⚡ Best class JUST for pain management
👶 Best Postpartum-Only Prep
❤️🧡💛💚💙💜 My favorite class is here.
Now is the time to get started!
Not sure we’re a good fit check out my free class — It’s your first step towards being your own birth boss.




Leave a Reply